Blog
Management of CaHA Vascular Complications: The 2026 Expert Consensus & Emergency Protocol
Author
Xie
Published
Category
CaHA Filler
Master CaHA (Radiesse) vascular occlusion management. 2024 expert consensus on 60-min vision loss protocols, necrosis care, and high-dose hyaluronidase.


Author
Xie
An esteemed medical aesthetics expert with 40 years of profound experience in the field. With decades of expertise in non-invasive procedures, anti-aging science, and advanced dermatological solutions, the author is dedicated to sharing insights that connect clinical innovation with real-world patient results. Passionate about advancing safe, effective, and high-impact aesthetic treatments for a global clientele.
What’s better than insider perks, pro tips, and surprises?
Sign up to get the most recent blog articles in your email every week.
Join now.
Our company’s main product lines include HA (Hyaluronic Acid) fillers, CaHA (Calcium Hydroxylapatite) fillers, PLLA (Poly-L-Lactic Acid) biostimulators, and other advanced aesthetic solutions, all developed and manufactured by trusted partner facilities with whom we have maintained long-term, stable collaborations.
I help them with sales and export operations, while our company also provides sourcing and procurement services in China to help international clients solve supply-related challenges. If you need assistance with procurement, please feel free to contact us.
1. The Physics of Prevention: Why the "0.1 mL Rule" is Absolute
The consensus highlights a critical biomechanical threshold: the 0.1 mL bolus.
1.1 The "Column of Fluid" Mechanism
When an injector applies pressure to a syringe, the filler acts as a solid column of fluid. If the needle tip is intra-arterial, the pressure of the injection can easily exceed the patient's mean arterial pressure (MAP).
Retrograde Flow: A bolus larger than 0.1 mL creates enough hydraulic force to push the filler backward (retrograde) through the arterial system until it reaches a bifurcation (such as the junction of the supratrochlear and ophthalmic arteries).
The Result: Once the injector releases pressure, the patient's own blood flow pushes the filler forward (anterograde) into smaller distal branches, leading to widespread "shower" embolization or total vision loss.
1.2 The "Aspiration Myth" in High-Viscosity Fillers
Aspiration is technically flawed with CaHA. Its high G' (elasticity) and viscosity mean that even if the needle is in a vessel, the resistance within the narrow lumen of a 27G or 30G needle often prevents blood from entering the syringe. A negative aspiration with CaHA is clinically meaningless.
2. Advanced Anatomy: The 3D High-Risk Matrix
High-Risk Region | Dominant Artery | Anatomical Nuance | Strategy |
|---|---|---|---|
Glabellar Complex | Supratrochlear / Supraorbital | Extensive anastomoses with the Ophthalmic Artery. | ABSOLUTE CONTRAINDICATION. Use HA or neuromodulators instead. |
Nasal Dorsum | Dorsal Nasal Artery | Terminal branches with poor collateral flow. | Supraperiosteal plane only. Use 22G blunt cannula; stay strictly midline. |
Nasolabial Fold | Facial / Angular Artery | Highly variable depth; becomes superficial near the alar base. | Avoid deep boluses at the pyriform aperture. Use retrograde fanning. |
Temple | Superficial Temporal (Frontal) | Artery is tethered to the temporoparietal fascia. | Avascular interfascial plane (between deep and superficial fascia). |
3. The "Pseudo-Paradox": Why Hyaluronidase Works for CaHA
A common misconception is that Hyaluronidase (Hyal) is useless for CaHA because CaHA is not an HA filler. The 2024 Consensus debunks this.
3.1 Interstitial Decompression
VO is not just about the "plug" in the vessel; it is about extravascular pressure.
Mechanism: Hyaluronidase dissolves the native hyaluronic acid in the skin's extracellular matrix (ECM).
Effect: This dramatically reduces interstitial fluid pressure and "thins" the surrounding tissue, allowing the artery to expand and potentially move the CaHA embolus further downstream into smaller, less critical vessels.
Anti-inflammatory Action: Hyal helps disperse pro-inflammatory mediators that aggregate around the ischemic site.
Consensus Dosage: 600 U per 0.1 mL of CaHA. High-dose pulse therapy is the current gold standard.
4. Diagnostic Differential: Bruising vs. Occlusion vs. Congestion
Immediate recognition is the difference between a minor scar and total necrosis.
Arterial Occlusion: Immediate "porcelain" blanching, followed by Livedo Reticularis (a geographic, violaceous, net-like pattern). Pain is usually sharp and sudden.
Venous Congestion: Occurs when the filler compresses veins. The skin looks dull, dark purple, or "swollen-red" rather than net-like. Pain is a dull, heavy throb. Capillary refill is often fast but the blood doesn't clear.
Ecchymosis (Bruising): Localized, does not follow a vascular distribution, and does not exhibit blanching or net-like mottling.
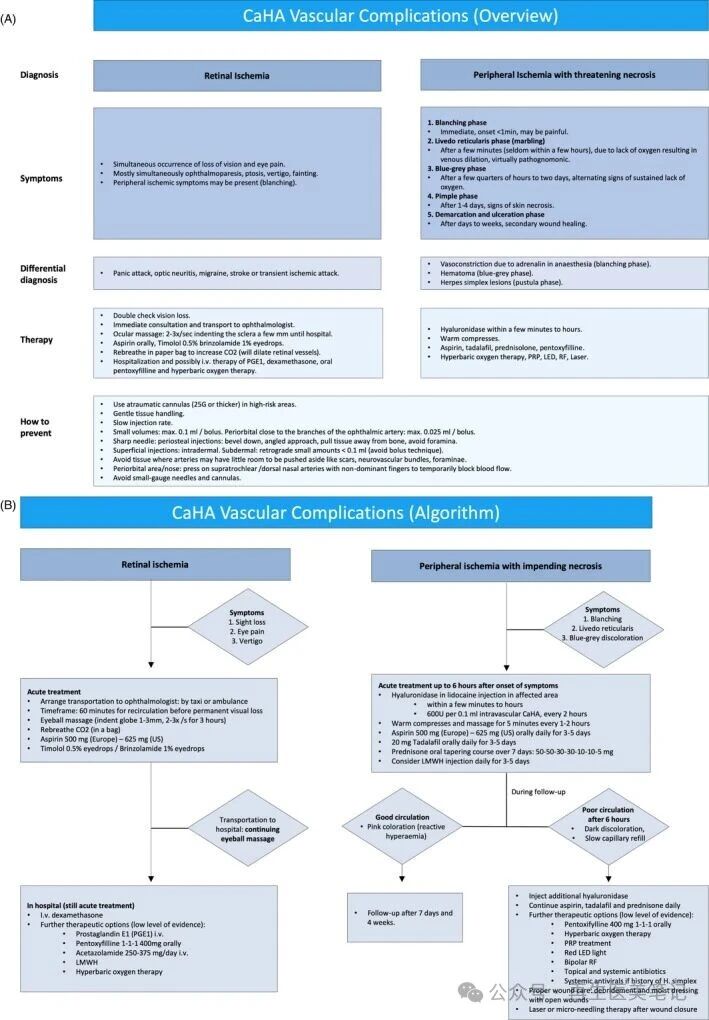
5. The Emergency "60-Minute" Vision Protocol
If a patient reports sudden darkness or excruciating ocular pain, the "Ophthalmic Clock" starts.
Immediate Ocular Massage: Apply firm pressure to the globe for 10-15 seconds, then release suddenly. Repeat 2-3 times per second. This "pumps" the aqueous humor to fluctuate intraocular pressure (IOP) and dislodge the embolus.
Vasodilation via Hypercapnia: Have the patient breathe into a paper bag. This increases pCO2pCO2, a potent natural vasodilator for the retinal arteries.
Chemical Intervention:
Aspirin (325-650 mg): Prevents the formation of a secondary blood clot around the CaHA microspheres.
Timolol 0.5% Drops: To lower IOP.
Referral: Immediate transport to an Ophthalmic Surgeon for potential anterior chamber paracentesis.
6. Sourcing & The "Crash Cart" Inventory
A world-class clinic must have a "Vascular Emergency Kit" ready for immediate use.
Hyaluronidase: Minimum 10-15 vials (1500 U/vial).
Aspirin: Non-coated (for faster absorption).
Nitroglycerin Paste (Optional/Controversial): Use only if Hyal is unavailable; avoid if using PDE5 inhibitors.
PDE5 Inhibitors: Sildenafil (50mg) or Tadalafil (20mg).
Warm Compresses: To induce localized vasodilation.
7. The 2026 "Cutting Edge": Ultrasound-Guided Rescue
The most significant evolution in VO management is Point-of-Care Ultrasound (POCUS).
Identification: High-frequency transducers (18-22 MHz) can identify the exact location of the CaHA bolus and the obstructed vessel.
Guided Dissolution: Instead of "flooding" the area with Hyal, the injector can use ultrasound to guide the needle directly to the perivascular space surrounding the occlusion, significantly increasing the success rate of decompression.
Source: PMC
FAQ: High-Intent Clinical Queries
Q: Can I use CaHA in the nose?
A: Yes, but only with extreme caution. The consensus recommends a supraperiosteal midline approach with a cannula. Never inject into the nasal tip or ala with CaHA due to the terminal nature of the arteries.
Q: Does CaHA cause more blindness than HA?
A: There is no evidence it is "more" dangerous, but because it cannot be dissolved (only the surrounding tissue can be decompressed), the margin for error is smaller.
Q: How long should I follow up after a VO event?
A: Daily for the first 7 days. Necrosis can be "staged," and secondary infections (like HSV activation) often appear on day 3 or 4.
Q: Is hyperdiluted CaHA (e.g., 1:1 or 1:3 ratios) safer than undiluted product regarding vascular risk?
A: While hyperdilution reduces the viscosity of the product, which theoretically lowers the risk of extrinsic compression (venous congestion caused by bulk pressure), it does not significantly lower the risk of intra-arterial embolism.
Q5: Why is there significant expert disagreement regarding the use of topical Nitroglycerin (NTG) paste?
A: Nitroglycerin was once a staple in vascular occlusion kits, but the 2024/2025 International Consensus expresses extreme caution for three primary reasons:
The "Steal Phenomenon": NTG is a potent vasodilator. In an ischemic zone, it may dilate neighboring healthy vessels, effectively "stealing" blood flow away from the already compromised central ischemic area and worsening the necrosis.
Masking of Symptoms: NTG frequently causes severe headaches, dizziness, and localized redness. These side effects can mask the early signs of cerebral infarction (stroke) or systemic distress, which are critical to monitor after a facial arterial event.
Fatal Drug Interactions: The consensus recommends PDE5 inhibitors (like Sildenafil or Tadalafil) as a first-line oral vasodilator. NTG is strictly contraindicated if a patient has taken a PDE5 inhibitor, as the combination can lead to life-threatening, refractory hypotension.
Advice: Only consider NTG as a last resort if hyaluronidase and oral vasodilators are unavailable, and only if the use of PDE5 inhibitors has been definitively ruled out.
Other Blogs

