Blog
CaHA/CMC Filler: Material Science, Porous Bio-Synthesized Advances & Nasal Shaping Performance
Author
Xie
Published
Category
CaHA Filler
Explore CaHA/CMC filler science: porous CaHA microspheres, CMC rheology, injection performance, and nasal shaping considerations.


Author
Xie
An esteemed medical aesthetics expert with 40 years of profound experience in the field. With decades of expertise in non-invasive procedures, anti-aging science, and advanced dermatological solutions, the author is dedicated to sharing insights that connect clinical innovation with real-world patient results. Passionate about advancing safe, effective, and high-impact aesthetic treatments for a global clientele.
What’s better than insider perks, pro tips, and surprises?
Sign up to get the most recent blog articles in your email every week.
Join now.
Our company’s main product lines include HA (Hyaluronic Acid) fillers, CaHA (Calcium Hydroxylapatite) fillers, PLLA (Poly-L-Lactic Acid) biostimulators, and other advanced aesthetic solutions, all developed and manufactured by trusted partner facilities with whom we have maintained long-term, stable collaborations.
I help them with sales and export operations, while our company also provides sourcing and procurement services in China to help international clients solve supply-related challenges. If you need assistance with procurement, please feel free to contact us.
The landscape of injectable fillers has moved far beyond simple "volume replacement." In 2026, the focus has pivoted toward biostimulatory regeneration—a field where the synergy between Calcium Hydroxylapatite (CaHA) and Sodium Carboxymethyl Cellulose (CMC) remains the undisputed gold standard.
With nearly two decades of clinical validation, this "Classic Duo" is undergoing a green revolution. By leveraging bio-synthetic technology to transform discarded seashells into high-purity, porous microspheres, the industry has unlocked a new level of neocollagenesis.
1. The Evolution: From Bone Grafting to "Green" Bio-Stimulation
Historically, CaHA was the domain of orthopedics. However, its transition into aesthetics—specifically when paired with the rheological prowess of CMC—has redefined facial contouring.
The 2006 Milestone: The first FDA approval of the 30% CaHA and 70% CMC ratio established the benchmark for "Immediate Lift + Long-term Regeneration."
The 2026 Innovation: Current bio-synthetic methods (Hydrothermal Synthesis) utilize waste oyster shells. This isn't just about sustainability; the resulting microporous structure offers a higher surface area-to-volume ratio, significantly accelerating fibroblast adhesion compared to traditional solid microspheres.
Industry Insight: The transition from synthetic to bio-derived CaHA reflects a broader market demand for "Biocompatible Circularity," where efficacy meets environmental ethics.
2. Technical Synergy: Why the 30/70 Ratio Works
The CaHA/CMC complex operates as a biphasic system. Understanding its rheological and biological interplay is critical for high-end product positioning.
The Physics of Projection
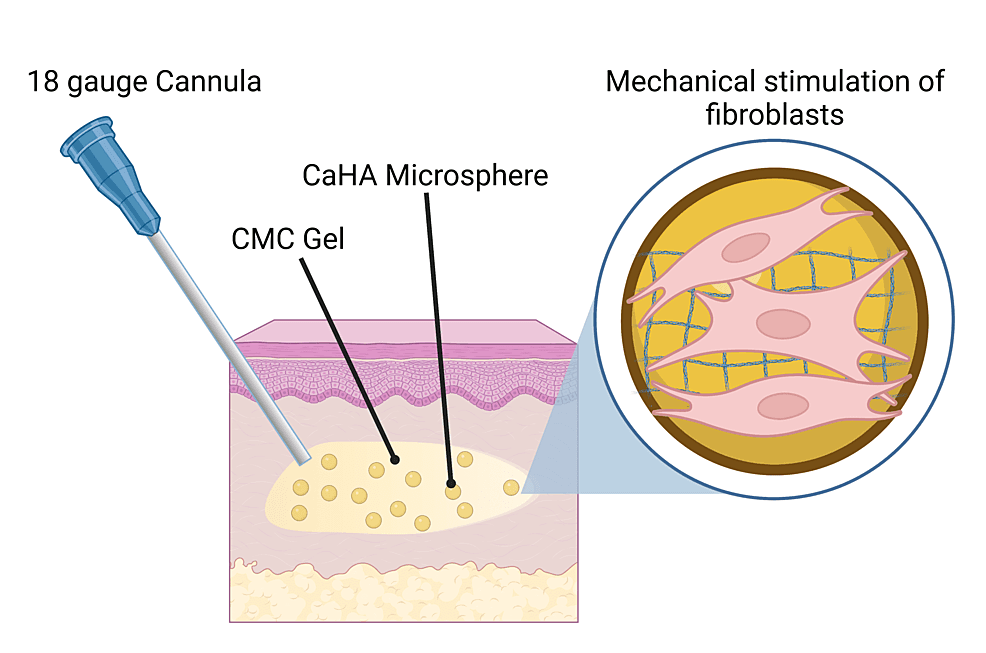
CMC serves as the carrier, providing a non-Newtonian, shear-thinning fluid behavior. This ensures that despite the high microsphere load, the injection remains smooth and predictable. Once injected, the CMC provides the Instant Volumization that patients crave.
The Biology of Scaffolding
As the CMC carrier degrades over 6–8 weeks, the CaHA microspheres (25–45μm) form a stable scaffold. This triggers a mechanical transduction response in fibroblasts, leading to the production of Type I Collagen and Elastin.
Key Performance Metrics (2026 Standards)
Parameter | Technical Specification | Clinical Benefit |
Storage Modulus (G') | 58.6 – 68.9 kPa | Superior lifting capacity & resistance to displacement |
Microsphere Diameter | 20 – 60 μm | Optimized for safety (prevents phagocytosis & embolization) |
Degradation Profile | Biphasic (Weeks for CMC / 18-30 Mo for CaHA) | Smooth transition from filler to natural tissue |
Calcium/Phosphate Ratio | 1.65 | Mimics natural bone mineralogy for peak biocompatibility |
3. The Litmus Test: Non-Surgical Rhinoplasty
Nasal contouring is widely considered the most demanding application for any regenerative material. It requires a delicate balance of High G' (for structural support) and Extreme Precision (to avoid vascular compromise).
Why CaHA/CMC is Dominating the Nasal Segment
Unlike Hyaluronic Acid (HA), which can sometimes lead to "widening" of the nasal bridge due to its hydrophilic nature, CaHA/CMC is highly cohesive and does not attract excess water. This allows for:
Bony Support: Injection at the supraperiosteal level creates a "liquid implant" effect.
Edge Definition: The high viscosity allows for sharp, crisp definition of the nasal tip and bridge.
Clinical Protocol: The "Less is More" Philosophy
The Layering Technique: Practitioners are now favoring 25G blunt cannulas via a single entry point at the nasal tip. This significantly mitigates the risk of intravascular injection in the high-risk angular artery zone.
Micro-Droplet Bolus: Deploying amounts $< 0.05$ mL per point prevents tissue over-expansion and maintains the integrity of local blood supply.
4. Market Landscape: The 2026 "Regulatory Dividend"
The global market for CaHA-based fillers is projected to reach $750M+ (approx. 4.87B RMB) by 2031, with China being the primary growth engine.
Policy Tailwinds: In 2025, the inclusion of "Hydroxylapatite-based Materials" into official medical pricing catalogs (such as China’s NMPA and local insurance guidelines) has moved these products from "niche luxury" to "mainstream medical necessity."
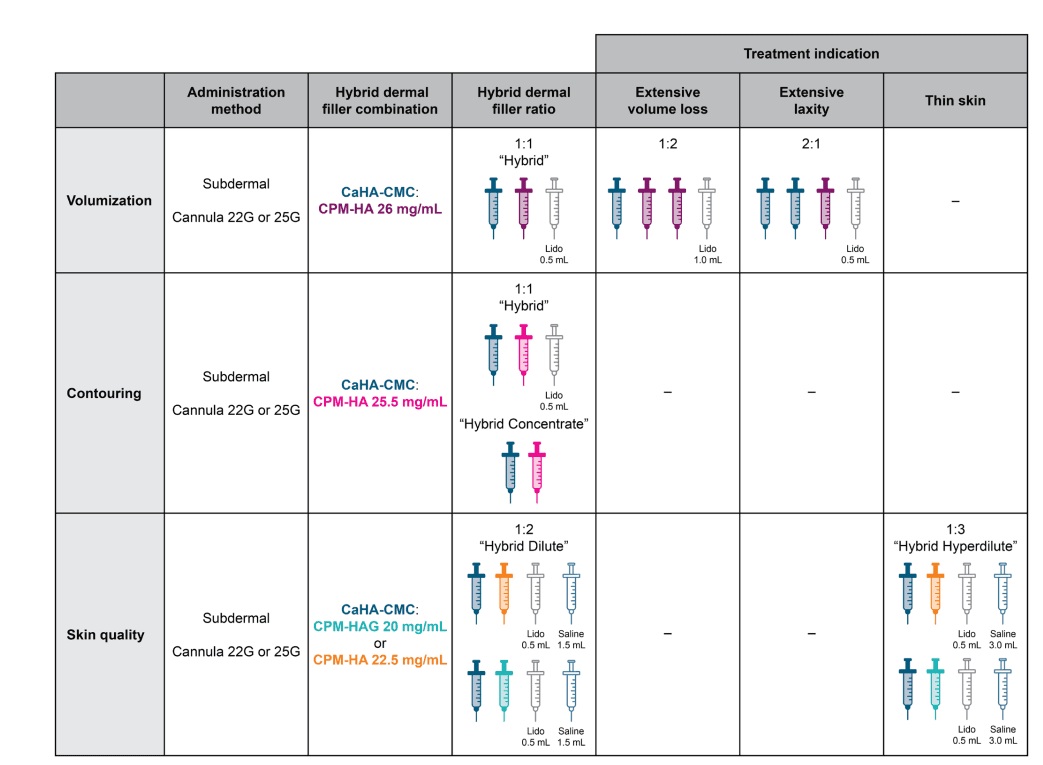
The Rise of Hybrids: A significant trend in 2026 is the 1:1 "Hybrid Filler"—mixing CaHA/CMC with Cohesive Polydensified Matrix Hyaluronic Acid (CPM-HA). This offers the hydration of HA with the structural longevity of CaHA.
5. Strategic Advantage for Brands and Manufacturers
For B2B stakeholders, the value proposition of the CaHA/CMC complex lies in differentiation:
Customization: We now offer adjustable porosity and particle sizing (20–60μm), allowing brands to create "Nose-Specific" or "Hand-Specific" formulations.
Evidence-Based Marketing: Success in 2026 relies on providing full toxicological data and in vivo neocollagenesis proof. Our bio-synthetic CaHA provides a cleaner, more consistent profile for NMPA/FDA submissions.
Conclusion: The Future is Bio-Integral
The CaHA/CMC complex is no longer just a "filler"—it is a sophisticated tool for bio-architectural restoration. By combining the wisdom of a 20-year-old classic with the innovations of 2026 bio-synthesis, the industry is finally achieving the dream of "invisible" and "sustainable" aging.
FAQ
Q1: What is a CaHA/CMC filler?
A: It’s a two-component dermal filler system combining calcium hydroxylapatite (CaHA) microspheres with a CMC (sodium carboxymethylcellulose) gel carrier, designed to provide early structural support and longer-term tissue remodeling cues.
Q2: What role does CMC play beyond “holding” the microspheres?
A: CMC primarily shapes rheology (injectability and stability) and influences how microspheres distribute after placement. It helps maintain consistency and early mechanical behavior.
Q3: What’s the benefit of porous bio-synthesized CaHA microspheres?
A: Porosity can increase micro-scale interactions by changing surface characteristics and tissue contact. Buyers should verify this with material characterization and QC documentation, not only with marketing claims.
Q4: Why is nasal shaping considered a high-demand use case?
A: Nasal shaping requires stable support and predictable placement in a region with complex anatomy and movement. Clinics should prioritize precision positioning and maintain risk preparedness protocols.
Q5: Is CaHA/CMC visible on imaging?
A: CaHA is generally described as being radiopaque due to its mineral content. The exact imaging appearance depends on the device and imaging modality—confirm using product documentation or published imaging studies.
Q6: What should clinics have ready for rare vascular complications?
A: Clinics should maintain a time-critical emergency protocol, trained staff, and an established referral pathway for ophthalmology/appropriate emergency care, aligned with expert consensus and local clinical standards.
Other Blogs

